



Conventional and Biological Disease-Modifying Antirheumatic Drugs in Chronic Kidney Disease and Hemodialysis
https://doi.org/10.46856/grp.10.e181
Cite as:
Santacruz Devia JC, Mantilla MJ, Pulido S, Varela DC, Agudelo CA, Londoño J. Conventional and Biological Disease-Modifying Antirheumatic Drugs in Chronic Kidney Disease and Hemodialysis. Global Rheumatology. Vol 5/ Ene - Jun [2024] Available from: https://doi.org/10.46856/grp.10.e181
Diagrama de flujo 1. Diagrama de búsqueda
{kind=link}
Tabla 1. Modificaciones de las dosis de los FARMES sintéticos convencionales sugerida según los niveles de evidencia
{kind=link}
Tabla 2. Modificaciones de las dosis de los FARMES sintéticos convencionales dirigidos y biológicos sugerida según los niveles de evidencia
{kind=link}
1395 Views
License
This is an open-access article distributed by the terms of the Creative Common Attribution License (CC-BY NC-4). The use, distribution or reproduction in other forms is permitted, provided the original author(a) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with this terms.
Conventional and Biological Disease-Modifying Antirheumatic Drugs in Chronic Kidney Disease and Hemodialysis
Advanced chronic kidney disease and the different modalities of renal replacement therapies have been a great limitation when prescribing the different conventional and biological therapies used for the treatment of different autoimmune diseases. Many of them persist with great activity, requiring the use of other types of medications such as glucocorticoids or non-steroidal anti-inflammatory drugs, further perpetuating their adverse effects. Addditionally, most clinical studies have excluded patients with chronic kidney disease and the evidence for continuing biological treatments in this scenario is based on pharmacokinetic properties or case reports where the outcomes have been favorable. The lack of knowledge and the absence of clear guidelines for decision-making regarding starting conventional or biological therapy in this context generate a lack of continuity in the prescription of treatments, which decreases the therapeutic response and negatively affects the quality of life. from the patients. For this reason, a narrative review is carried out with the aim of establishing a practical consensus that unifies the recommendations for each of the treatments most frequently used in the control of various autoimmune diseases in patients with advanced chronic kidney disease.
The kidney has often been affected by various prevalent autoimmune diseases, such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and systemic sclerosis (SSc) (1). This may be due both to damage associated with disease activity and to chronic deterioration linked to the use of certain immunosuppressive drugs (2). In addition, the frequent use of nonsteroidal anti-inflammatory drugs (NSAIDs) has also been identified as a contributing factor to the progression of kidney disease, associated with other comorbidities such as diabetes and hypertension (3). Historically, chronic kidney disease has represented a significant limitation for the use of disease-modifying antirheumatic drugs (DMARDs), both synthetic and biologic, due to the increased risk of toxicity posed by some of them, making their use unsafe in this context. It is also relevant to highlight the notable scarcity of clinical studies investigating the efficacy and safety of DMARDs in patients with chronic kidney disease (CKD) and undergoing dialysis (4). It is well known that CKD is characterized by a chronic inflammatory state, supported by the increased levels of several growth factors and inflammatory mediators, such as C-reactive protein, tumor necrosis factor, and monocyte chemoattractant protein-1 (5). This suggests that systemic inflammation plays a crucial role in the deterioration of kidney function, highlighting the need to block these mediators to mitigate kidney damage (6). This phenomenon is evident in cases of secondary amyloidosis, especially in rheumatoid arthritis (RA) and ankylosing spondylitis, where the use of tumor necrosis factor inhibitors (TNFi) is required despite the preexisting established kidney damage (7). Since this paradox remains, the current prescription of DMARDs in CKD is based on the pharmacokinetic and pharmacodynamic characteristics of each drug, rather than on evidence derived from clinical trials (8). Furthermore, several questions remain, such as: the great discrepancy in the recommendations regarding dose adjustment of several DMARDs based on glomerular filtration rate (GFR); the lack of knowledge about whether the dose adjustments and metabolism of DMARDs differ depending on each autoimmune disease; the uncertainty about whether there are variations in plasma concentrations due to frequent drug interactions; and to what extent the benefit of continuing each DMARD can be defined if kidney disease progresses (9).
Methodology
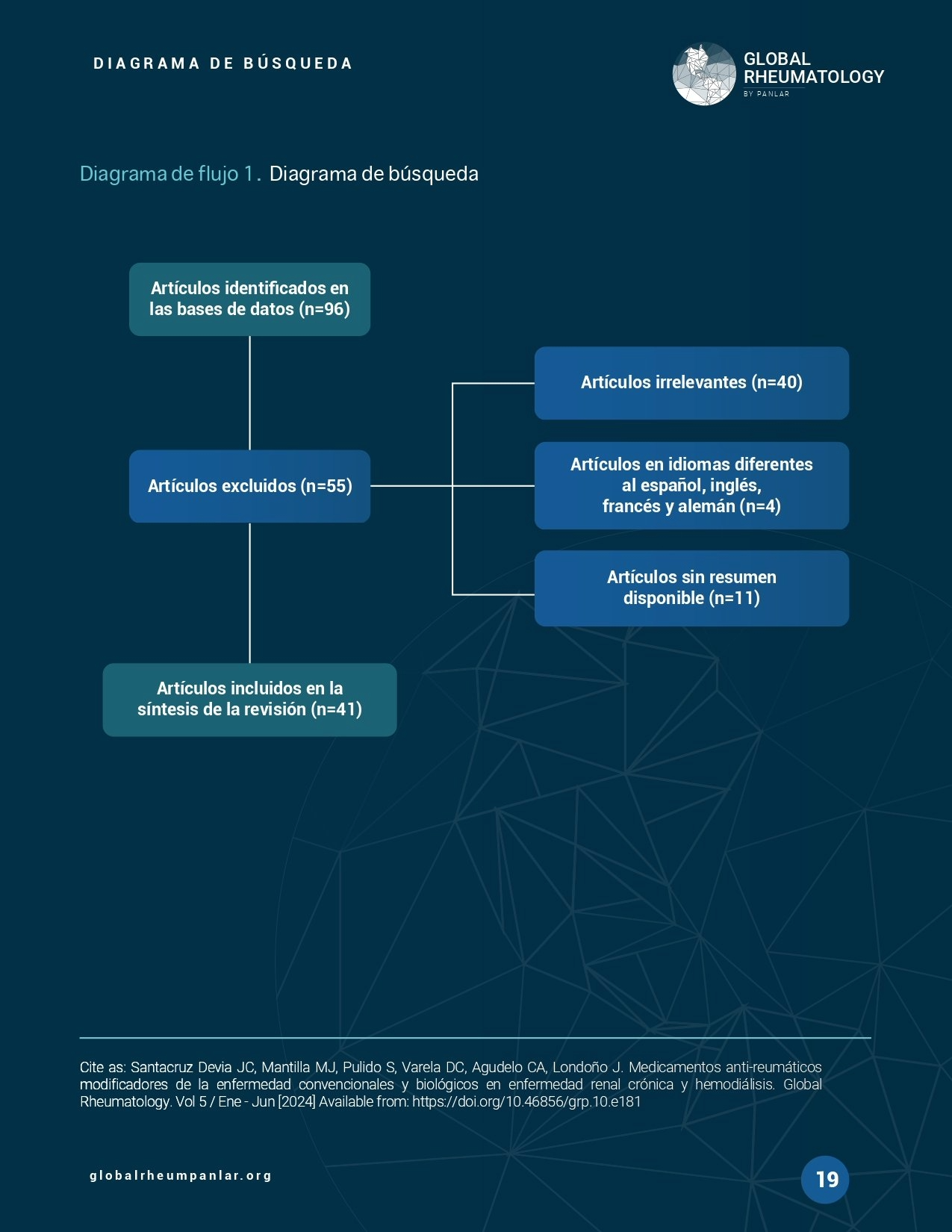
A non-systematic narrative review of the literature was conducted in English, French, Spanish, and German. It is important to note that no clinical studies were identified to justify a systematic review or meta-analysis. The purpose of this review was to gather the most representative available information from articles referenced in primary databases such as PubMed, Embase, and Google Scholar. The MESH (Medical Subject Headings) terms used were: “Chronic kidney disease,” “Conventional synthetic disease-modifying antirheumatic drugs,” “Tumor necrosis factor inhibitors,” “JAK inhibitors,” “Cyclophosphamide,” and “Rituximab”; these were combined using Boolean operators (AND, OR). The search was extended to include other commonly used drugs such as secukinumab, ixekizumab, guselkumab, and abatacept, but no representative data were found to support a recommendation. Below is a flow diagram detailing the search strategy (Diagram 1).
Conventional synthetic disease-modifying antirheumatic drugs
Methotrexate
Methotrexate (MTX) is a prodrug that becomes active once polyglutamated within the cell. This process occurs gradually and can take up to 27.5 weeks to reach a steady state. This time frame explains the delay in achieving the plateau of therapeutic response (10). The drug is mainly eliminated via the renal route, with approximately 80–90% excreted unchanged in the urine. This characteristic explains why any reduction in GFR leads to increased serum levels of the drug and, consequently, a higher risk of myelotoxicity (11). MTX is contraindicated when GFR is below 30 ml/min; if GFR is between 30–59 ml/min, a lower starting dose (7.5–10 mg weekly) is recommended. Other authors suggest contraindicating the drug when GFR is below 45 ml/min, as the drug’s elimination half-life doubles from 11 to 22.4 hours compared to patients with normal renal function, whereas at a GFR of 45–60 ml/min, it only doubles to 13.5 hours (12). Cases of methotrexate toxicity (including death) have been reported in patients receiving hemodialysis, even at low doses, and higher doses have required the use of leucovorin or extended dialysis with high-flux membranes to facilitate elimination (13)(14). It is also contraindicated in patients requiring peritoneal dialysis, although it may be prescribed (with a 50% dose reduction) in cases requiring continuous renal replacement therapy (15).
Leflunomide
The pharmacokinetics of leflunomide in CKD are largely unknown. Some studies have shown that teriflunomide (the active metabolite of leflunomide) was similar after administration of 100 mg of leflunomide in three patients undergoing peritoneal dialysis and reduced in patients on hemodialysis compared to healthy controls. Despite this, the free fraction of the drug in dialysis patients was higher (1.51%) compared to the 0.62% observed in controls. This finding suggests the need for closer monitoring when considering leflunomide administration in cases of advanced renal insufficiency (16). Leflunomide is positioned as the first-line drug in cases of advanced renal insufficiency due to its favorable pharmacokinetic properties. It is important to consider other possible side effects, such as poor blood pressure control, delayed wound healing, and an increased risk of infections (17).
Sulfasalazine
Nephrotoxicity associated with sulfasalazine (SSZ) is predominantly attributed to interstitial nephritis, whether acute or chronic. This complication may manifest within the first 12 months of treatment or even after several years. It is important to note that interstitial nephritis is idiosyncratic and is not usually directly related to the administered dose (18). Drug-induced acute kidney injury secondary to crystalluria has also been reported; therefore, discontinuation of the medication in patients presenting with nephrotoxicity is considered necessary.
Supportive measures such as hydration or the prescription of glucocorticoids will depend on the underlying mechanism causing the acute kidney injury (19). It is important to emphasize that 5-aminosalicylic acid (5-ASA) preparations, such as SSZ and mesalazine, may rarely induce allergic interstitial nephritis. This condition shows recovery in up to 85% of cases following drug discontinuation. A study conducted in patients with inflammatory bowel disease showed a decrease in GFR among those treated with 5-ASA preparations. In this regard, the loss was more pronounced in the group receiving SSZ (−19.5±24.3 ml/min) compared to mesalazine (−7.5±24.7 ml/min), possibly attributable to longer treatment duration in the former group (20). In patients with autoimmune diseases and CKD, it is recommended to start treatment with the lowest dose within the usual range when GFR is below 60 ml/min. Although there is limited data on the safety of SSZ use in patients with end-stage renal disease, it is known that SSZ is not dialyzable, as it binds to plasma proteins in more than 99%. A daily dose of 1 gram has been shown to be well tolerated in patients requiring hemodialysis. However, there is insufficient data on the efficacy or safety of higher doses. There is a need to gather more information to assess the suitability of SSZ treatment in this specific population (21).
Antimalarials (Chloroquine/Hydroxychloroquine)
After oral administration, chloroquine (CQ) and hydroxychloroquine (HCQ) are rapidly and almost completely absorbed. They distribute to tissues in variable concentrations due to their large volume of distribution. Peak blood levels are reached after approximately 4 hours for CQ and between 2 to 6 hours for HCQ. In the blood, about 50% of CQ/HCQ binds to plasma proteins. In solid organs such as the heart, lungs, kidneys, and liver, tissue levels are significantly higher (10 times greater) compared to plasma. The active ingredient has a high affinity for melanin-containing tissues (mainly the skin and eyes) (22). The half-life of CQ and HCQ ranges from 40 to 50 days, and their main metabolites are monodesethyl chloroquine and monodesethyl hydroxychloroquine. It is advised to reduce the dose of HCQ and CQ by 50% when GFR is below 30 ml/min. The incidence of ocular adverse effects tends to increase as renal function declines. In cases of renal insufficiency, HCQ is preferred due to its lower renal elimination, as monodesethyl hydroxychloroquine is primarily excreted through feces, with less renal elimination. Some authors suggest reducing the dose by 50% only when GFR is below 10 ml/min and when prolonged use is anticipated. This adjustment is also recommended for patients undergoing hemodialysis and peritoneal dialysis. However, in patients on continuous renal replacement therapy, dose reduction is not necessary (23).
Azathioprine
Azathioprine is converted into the active metabolite 6-mercaptopurine in the liver and erythrocytes. Most of its metabolites are biologically inactive, with the exception of 6-mercaptopurine, which is partially excreted renally, and 6-thioinosinic acid, which is formed from 6-mercaptopurine and remains intracellular (24). For this reason, when the GFR is in the range of 10–50 ml/min, the azathioprine dose should be reduced to 75% of the standard dose. Other authors suggest administering 75% of the dose in situations where the GFR ranges between 10–30 ml/min (24). In cases of GFR below 10 ml/min or when the patient is undergoing hemodialysis, it is recommended to reduce the dose to 50% and to take it after each session, since approximately 48% of the drug is eliminated by dialysis over an 8-hour period (25).
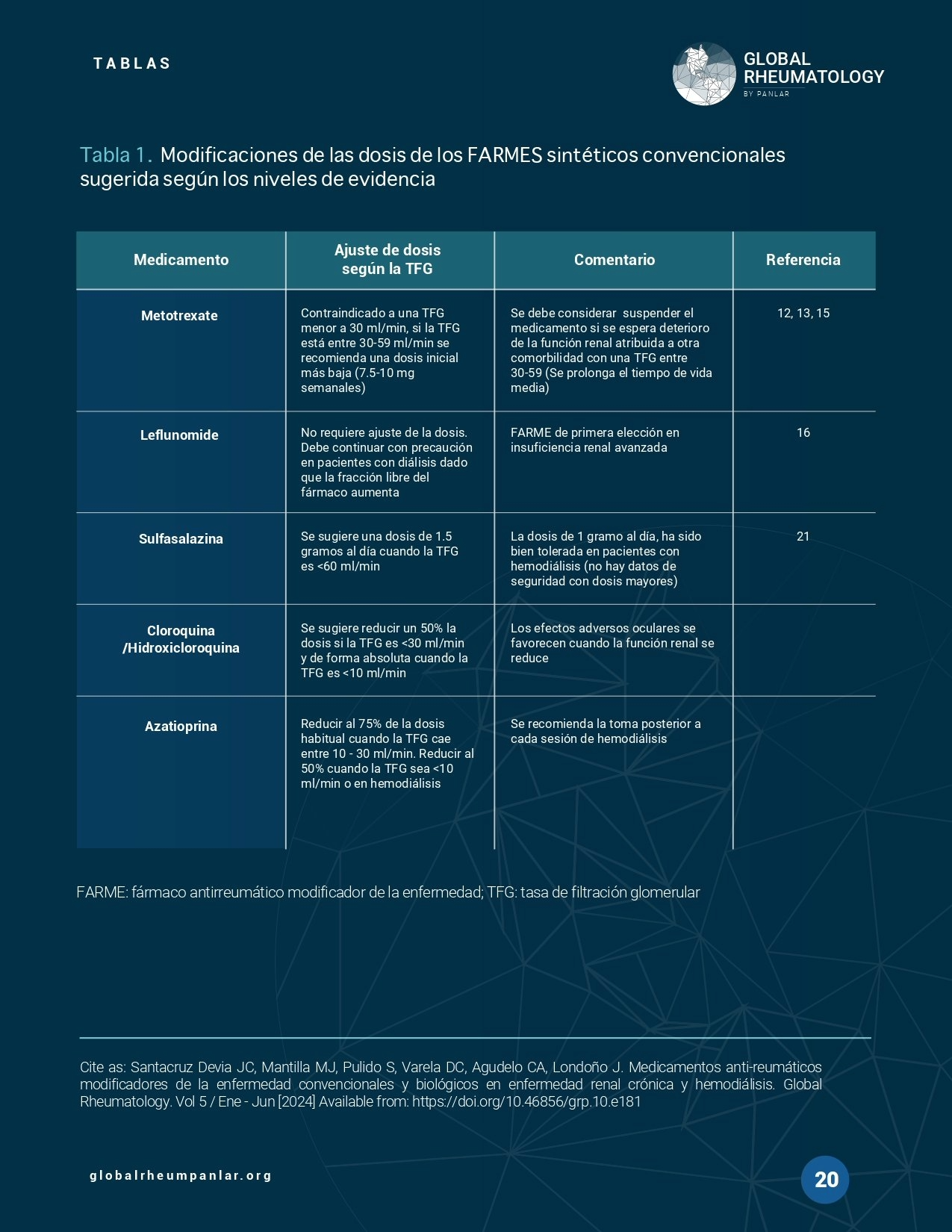
The following table presents the suggested dose modifications of conventional synthetic drugs according to levels of evidence (Table 1).
Tumor Necrosis Factor Inhibitors
Etanercept
The exact clearance mechanism of etanercept is unknown, although metabolism is believed to occur through peptide pathways, likely mediated via the Fc binding in the reticuloendothelial system (26). The resulting amino acids from metabolism are recycled or eliminated through bile or urine. The immunoglobulin structure gives the drug a half-life of 3 to 4.8 days. A case report in renal failure showed that the half-life of etanercept was slightly prolonged, whereas another study including 6 patients on hemodialysis found that the pharmacokinetics were unchanged compared to controls (27). Small case series addressing treatment with etanercept at a dose of 25 mg once or twice weekly in end-stage renal disease have not documented adverse effects (28)(29).
Golimumab, Adalimumab, and Certolizumab
There are no pharmacokinetic data on the use of golimumab, adalimumab, or certolizumab in advanced renal failure, but it has been proposed that antibodies are hydrolyzed by lysosomes, undergoing intracellular catabolism without requiring renal involvement. Clinical data exist only for adalimumab from a retrospective study that showed no serious infections or other side effects in patients with a GFR of 41.6 ml/min (n=39) compared to a control of 83 ml/min (n=26), including 2 patients on dialysis (30).
Janus Kinase Inhibitors
Tofacitinib
Tofacitinib is a Janus kinase (JAK) inhibitor that is primarily metabolized in the liver via cytochrome P450 enzymes 3A4 and 2C19. Seventy percent of clearance occurs through the hepatic route, and the remaining 30% is excreted renally (31). In RA studies, patients with an eGFR < 40 or 50 mL/min were excluded. There is limited data on the use of tofacitinib in patients with an eGFR < 40 mL/min; therefore, it should not be used in advanced renal insufficiency, and if necessary, the dose should be reduced by 50%. Additionally, if it is absolutely necessary to continue treatment in end-stage renal disease, it is recommended to administer the drug after each dialysis session, as part of it is dialyzable (31).
Baricitinib
The recommended dose of baricitinib is 4 mg once daily. A dose of 2 mg per day is recommended for patients over 75 years of age and for those with a history of chronic or recurrent infections (32). The total body clearance of baricitinib is 8.9 L/h, with a half-life of nearly 12 hours. The drug's technical sheet recommends a 2 mg dose in patients with an eGFR between 30 and 60 mL/min. The use of baricitinib is not recommended in patients with a creatinine clearance < 30 mL/min (33).
Upadacitinib
Upadacitinib is a JAK inhibitor with greater selectivity for JAK1 than for JAK2, JAK3, or TYK (34). Weight, sex, race, age, mild to severe renal insufficiency, and mild to moderate hepatic insufficiency (Child-Pugh A or B) do not affect its safety (35). One study showed that the renal clearance of upadacitinib decreased progressively with increasing severity of renal insufficiency (5.6 L/h in subjects with normal renal function and 1.06 L/h in subjects with severe renal insufficiency). Population pharmacokinetic analyses of upadacitinib in patients with rheumatoid arthritis showed that those with mild to moderate renal insufficiency (with an average creatinine clearance of 40 mL/min) experienced a 16% to 32% increase in plasma concentrations compared to controls (36). Despite this, the overall renal clearance of the drug is very low and no dose adjustment is necessary, unless the eGFR is below 30 mL/min, in which case it is contraindicated (37).
Cyclophosphamide and Rituximab
Cyclophosphamide, which is itself inactive, is converted in the liver into the active metabolites 4-hydroxycyclophosphamide and aldophosphamide via CYP2B6 and CYP3A4. About 20-25% of cyclophosphamide is excreted unchanged in the urine. In the presence of renal insufficiency, its clearance significantly decreases. Cyclophosphamide binds slightly to plasma proteins, whereas its metabolites bind up to 50%. The metabolites are also primarily excreted renally (38). For this reason, a dose adjustment of 75% of the usual dose is necessary when eGFR is between 10–30 mL/min, and it should be reduced to 50% when eGFR is below 10 mL/min. Cyclophosphamide shows moderate dialyzability (20–50%), so maintaining a 50% dose adjustment is recommended in intermittent hemodialysis situations. In these cases, it is advised to administer the next dose during the following session, allowing at least 12 hours to pass before the subsequent application (39). Rituximab is not removed during hemodialysis, so it can be administered at standard doses in patients with advanced end-stage renal disease without requiring any adjustment (40).
Tocilizumab
A case report was identified of a 64-year-old Japanese woman with RA who achieved low disease activity as measured by DAS28-CRP and was able to reduce glucocorticoid use with the administration of tocilizumab while on hemodialysis at a dose of 8 mg/kg every 4 weeks, without any adverse effects reported from its use (41).
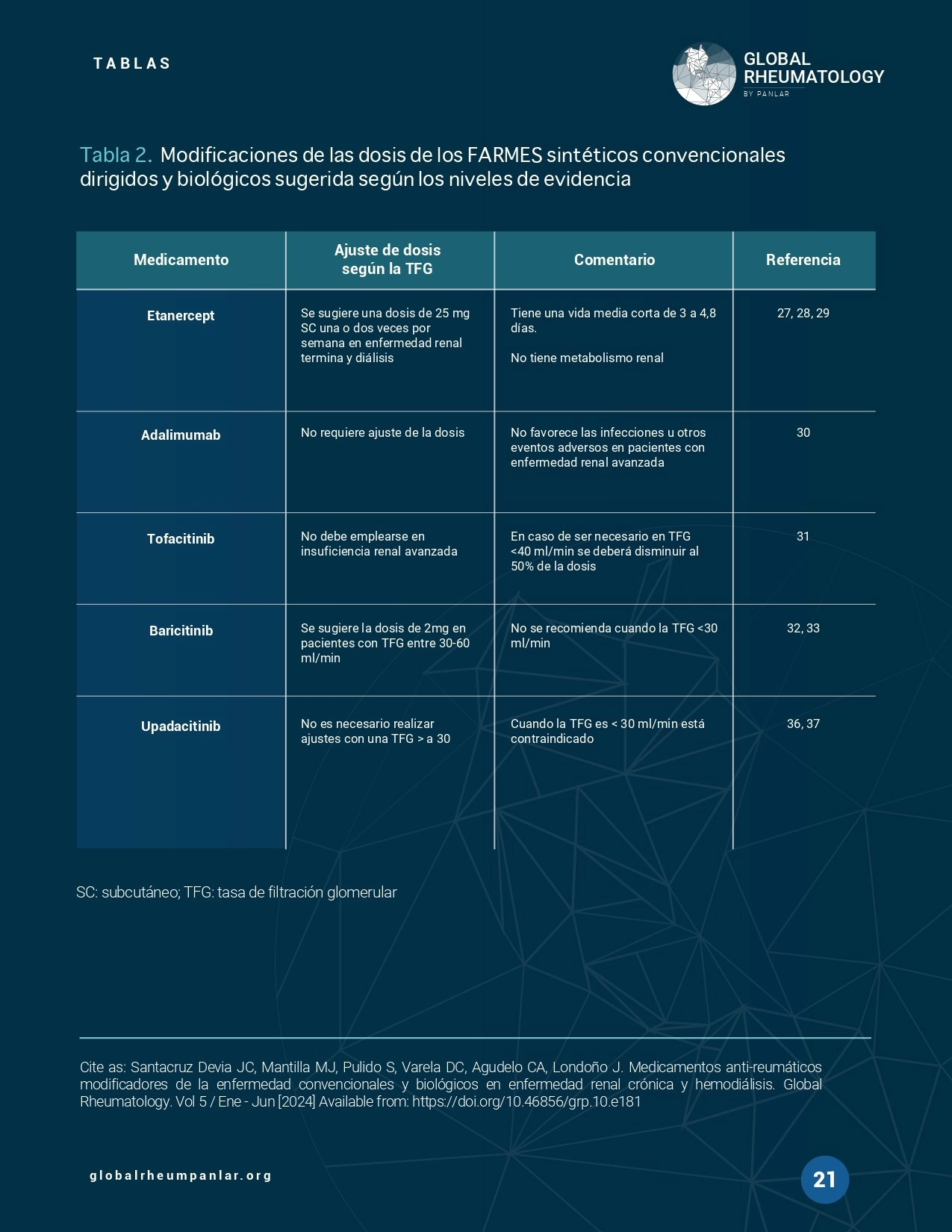
A table is presented below showing the suggested dose modifications for biologic DMARDs and targeted synthetic DMARDs according to levels of evidence (Table 2).
Although relevant pharmacological aspects of conventional synthetic DMARDs (csDMARDs) are known in daily clinical practice, the available information remains insufficient to issue recommendation grades with higher levels of evidence in patients with chronic kidney disease (CKD). Despite this, the currently available evidence was unified to provide safe and practical recommendations, based on pharmacological properties and, in some cases, on case reports with satisfactory outcomes. Leflunomide is the conventional synthetic drug that shows the greatest safety in patients with advanced-stage CKD, and most of these drugs require dosage adjustment according to glomerular filtration rate (GFR). TNF inhibitors, which undergo intracellular catabolism without depending on renal clearance, may be safe in this context. However, the reported cases with favorable outcomes have been mainly associated with etanercept and adalimumab. Regarding JAK inhibitors, upadacitinib does not require dose adjustment with GFR greater than 30 ml/min, while tofacitinib and baricitinib require adjustments in stage 3 CKD. Tofacitinib is the only JAK inhibitor that has been prescribed in some cases of patients undergoing hemodialysis. It is important to consider cyclophosphamide adjustment when GFR drops below 30 ml/min, due to the increased risk of adverse events, including bone marrow suppression, infections, increased malignancy risk, and hyponatremia. Rituximab, on the other hand, can be administered without contraindications at any stage of CKD.
As authors of this article, we certify that none of the materials in the manuscript (including tables and figures) have been previously published, nor are they included in any other document.
This article has not received specific funding from the public sector, commercial sector, or nonprofit organizations.
1. Castro LL, Lanna CCD, Rocha MP, Ribeiro ALP, Telles RW. Recognition and control of hypertension, diabetes, and dyslipidemia in patients with rheumatoid arthritis. Rheumatol Int [Internet]. 2018 Aug 15;38(8):1437–42. Available from: http://link.springer.com/10.1007/s00296-018-4084-3
2. Hernández-Negrín H, Ricci M, Mancebo-Sevilla JJ, Sanz-Cánovas J, López- Sampalo A, Cobos-Palacios L, et al. Obesity, Diabetes, and Cardiovascular Risk Burden in Systemic Lupus Erythematosus: Current Approaches and Knowledge Gaps—A Rapid Scoping Review. Int J Environ Res Public Health [Internet]. 2022 Nov 10;19(22):14768. Available from: https://www.mdpi.com/1660-4601/19/22/14768
3. Chiu H-Y, Huang H-L, Li C-H, Chen H-A, Yeh C-L, Chiu S-H, et al. Increased Risk of Chronic Kidney Disease in Rheumatoid Arthritis Associated with Cardiovascular Complications – A National Population-Based Cohort Study. Burdmann EA, editor. PLoS One [Internet]. 2015 Sep 25;10(9):e0136508.
Available from: https://dx.plos.org/10.1371/journal.pone.0136508
4. Freitas RV de, Godinho F. Rheumatoid Arthritis and Chronic Kidney Disease Under Dialysis – Are Anti-TNF an Option? Reumatol Clínica (English Ed [Internet]. 2022 Dec;18(10):623. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2173574322001629
5. Pecoits-Filho R, Heimbürger O, Bárány P, Suliman M, Fehrman-Ekholm I, Lindholm B, et al. Associations between circulating inflammatory markers and residual renal function in CRF patients. Am J Kidney Dis [Internet]. 2003 Jun;41(6):1212–8. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0272638603003536
6. Oberg BP, McMenamin E, Lucas FL, McMonagle E, Morrow J, Ikizler TALP, et al. Increased prevalence of oxidant stress and inflammation in patients with moderate to severe chronic kidney disease. Kidney Int [Internet]. 2004 Mar;65(3):1009–16. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0085253815497947
7. Tonelli M, Sacks F, Pfeffer M, Jhangri GS, Curhan G. Biomarkers of inflammation and progression of chronickidney disease. Kidney Int [Internet]. 2005 Jul;68(1):237–45. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0085253815508314
8. Goicoechea M, García de Vinuesa S, Quiroga B, Verdalles U, Barraca D, Yuste C, et al. Effects of pentoxifylline on inflammatory parameters in chronic kidney disease patients: a randomized trial. J Nephrol [Internet]. 2012;25(6):969–75. Available from: http://www.jnephrol.com/Navigator.action?cmd=navigate&urlkey=Abstract&t= JN&UidArticle=6B9C4C23-2D91-456E-AF06-B80B7190908E
9. Kim HW, Lee C-K, Cha H-S, Choe J-Y, Park E-J, Kim J. Effect of anti-tumor necrosis factor alpha treatment of rheumatoid arthritis and chronic kidney disease. Rheumatol Int [Internet]. 2015 Apr 8;35(4):727–34. Available from: http://link.springer.com/10.1007/s00296-014-3146-4
10. Dalrymple JM, Stamp LK, O’Donnell JL, Chapman PT, Zhang M, Barclay ML. Pharmacokinetics of oral methotrexate in patients with rheumatoid arthritis. Arthritis Rheum [Internet]. 2008 Nov;58(11):3299–308. Available from: https://onlinelibrary.wiley.com/doi/10.1002/art.24034
11. Dhillon GS, Chauhan S, Jalal Y, Ghobrial Y, Ahmed B. Low-Dose Methotrexate Toxicity Presenting as Pancytopenia. Cureus [Internet]. 2022 Dec 13; Available from: https://www.cureus.com/articles/126975-low-dose- methotrexate-toxicity-presenting-as-pancytopenia
12. Basile C, Montanaro A, Semeraro A. Should low‐ dose methotrexate therapy be prescribed to dialysis patients? Nephrol Dial Transplant [Internet]. 2002 Mar 1;17(3):530–1. Available from: http://academic.oup.com/ndt/article/17/3/530/1807745
13. Murashima M, Adamski J, Milone MC, Shaw L, Tsai DE, Bloom RD. Methotrexate Clearance by High-Flux Hemodialysis and Peritoneal Dialysis: A Case Report. Am J Kidney Dis [Internet]. 2009 May;53(5):871–4. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0272638609000821
14. Bennett WM, Aronoff GR, Morrison G, Golper TA, Pulliam J, Wolfson M, et al. Drug Prescribing in Renal Failure: Dosing Guidelines for Adults. Am J Kidney Dis [Internet]. 1983 Nov;3(3):155–93. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0272638683800602
15. Beaman JM, Hackett LP, Luxton G, Illett KF. Effect of Hemodialysis on Leflunomide Plasma Concentrations. Ann Pharmacother [Internet]. 2002 Jan 28;36(1):75–7. Available from: http://journals.sagepub.com/doi/10.1345/aph.1A127
16. Bergner R, Peters L, Schmitt V, Löffler C. Leflunomide in dialysis patients with rheumatoid arthritis—a pharmacokinetic study. Clin Rheumatol [Internet]. 2013 Feb 22;32(2):267–70. Available from: http://link.springer.com/10.1007/s10067-012-2122-1
17. Russo PA, Wiese MD, Smith MD, Ahern MJ, Barbara JA, Shanahan EM. Leflunomide for Inflammatory Arthritis in End-Stage Renal Disease on Peritoneal Dialysis: A Pharmacokinetic and Pharmacogenetic Study. Ann Pharmacother [Internet]. 2013 Mar 21;47(3):e15–e15. Available from: http://journals.sagepub.com/doi/10.1345/aph.1R542
18. Van Staa TP, Travis S, Leufkens HGM, Logan RF. 5-aminosalicylic acids and the risk of renal disease: A large British epidemiologic study☆. Gastroenterology [Internet]. 2004 Jun;126(7):1733–9. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0016508504003828
19. Gisbert JP, González-Lama Y, Maté J. 5-Aminosalicylates and renal function in inflammatory bowel disease. Inflamm Bowel Dis [Internet]. 2007 May;13(5):629–38. Available from: https://academic.oup.com/ibdjournal/article/13/5/629-638/4644696
20. Patel H, Barr A, Jeejeebhoy KN. Renal Effects of Long-Term Treatment with 5-Aminosalicylic Acid. Can J Gastroenterol [Internet]. 2009;23(3):170–6. Available from: http://www.hindawi.com/journals/cjgh/2009/501345/
21. Akiyama Y, Sakurai Y, Kato Y, Furuta E, Mimura T. Retrospective study of salazosulfapyridine in eight patients with rheumatoid arthritis on hemodialysis. Mod Rheumatol [Internet]. 2014 Mar 4;24(2):285–90. Available from: https://academic.oup.com/mr/article/24/2/285-290/6315752
22. Jallouli M, Galicier L, Zahr N, Aumaître O, Francès C, Le Guern V, et al. Determinants of Hydroxychloroquine Blood Concentration Variations in Systemic Lupus Erythematosus. Arthritis Rheumatol [Internet]. 2015 May;67(8):2176–84. Available from: https://onlinelibrary.wiley.com/doi/10.1002/art.39194
23. Chiowchanwisawakit P, Srinonprasert V, Nilganuwong S, Katchamart W, Koolvisoot A, Arromdee E, et al. Antimalarial-induced maculopathy: accuracy of Amsler grid as a diagnostic tool and risk factors. J Med Assoc Thai [Internet]. 2012 Feb;95 Suppl 2(2):S218-26. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22574553
24. Bach J-F, Dardenne M. THE METABOLISM OF AZATHIOPRINE IN RENAL FAILURE. Transplantation [Internet]. 1971 Oct;12(4):253–9. Available from: http://journals.lww.com/00007890-197110000-00003
25. Schusziarra V, Ziekursch V, Schlamp R, Siemensen HC. Pharmacokinetics of azathioprine under haemodialysis. Int J Clin Pharmacol Biopharm [Internet]. 1976 Dec;14(4):298–302. Available from: http://www.ncbi.nlm.nih.gov/pubmed/1002367
26. De Groot AS, Scott DW. Immunogenicity of protein therapeutics. Trends Immunol [Internet]. 2007 Nov;28(11):482–90. Available from: https://linkinghub.elsevier.com/retrieve/pii/S147149060700230X
27. Don BR, Spin G, Rose A, Nestorov I, Hutmacher M, Kaysen GA. The pharmacokinetics of etanercept in patients with end-stage renal disease on haemodialysis. J Pharm Pharmacol [Internet]. 2010 Feb 18;57(11):1407–13. Available from: https://academic.oup.com/jpp/article/57/11/1407/6147630
28. Mahmoud I, Gafsi L, Tekaya R, Saidane O, Sahli H, Abdelmoula L, et al. Inocuité et efficacité de l’étanercept lors d’une polyarthrite rhumatoïde compliquée d’insuffisance rénale terminale à propos d’un cas. Therapies [Internet]. 2015 May;70(3):311–2. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0040595716310733
29. Senel S, Kisacik B, Ugan Y, Kasifoglu T, Tunc E, Cobankara V. The efficacy and safety of etanercept in patients with rheumatoid arthritis and spondyloarthropathy on hemodialysis. Clin Rheumatol [Internet]. 2011 Oct 28;30(10):1369–72. Available from: http://link.springer.com/10.1007/s10067- 011-1782-6
30. Sumida K, Ubara Y, Suwabe T, Hayami N, Hiramatsu R, Hasegawa E, et al. Adalimumab treatment in patients with rheumatoid arthritis with renal insufficiency. Arthritis Care Res (Hoboken) [Internet]. 2013 Mar;65(3):471–5. Available from: https://onlinelibrary.wiley.com/doi/10.1002/acr.21800
31. Bannwarth B, Kostine M, Poursac N. A pharmacokinetic and clinical assessment of tofacitinib for the treatment of rheumatoid arthritis. Expert Opin Drug Metab Toxicol [Internet]. 2013 Jun 9;9(6):753–61. Available from: http://www.tandfonline.com/doi/full/10.1517/17425255.2013.789500
32. Assadiasl S, Fatahi Y, Mosharmovahed B, Mohebbi B, Nicknam MH. Baricitinib: From Rheumatoid Arthritis to COVID‐19. J Clin Pharmacol [Internet]. 2021 Oct 12;61(10):1274–85. Available from: https://onlinelibrary.wiley.com/doi/10.1002/jcph.1874
33. Markham A. Baricitinib: First Global Approval. Drugs [Internet]. 2017 Apr 13;77(6):697–704. Available from: http://link.springer.com/10.1007/s40265- 017-0723-3
34. Parmentier JM, Voss J, Graff C, Schwartz A, Argiriadi M, Friedman M, et al. In vitro and in vivo characterization of the JAK1 selectivity of upadacitinib (ABT-494). BMC Rheumatol [Internet]. 2018 Dec 28;2(1):23. Available from: https://bmcrheumatol.biomedcentral.com/articles/10.1186/s41927-018-0031- x
35. Duggan S, Keam SJ. Upadacitinib: First Approval. Drugs [Internet]. 2019 Nov 22;79(16):1819–28. Available from: http://link.springer.com/10.1007/s40265- 019-01211-z
36. Klünder B, Mohamed M-EF, Othman AA. Population Pharmacokinetics of Upadacitinib in Healthy Subjects and Subjects with Rheumatoid Arthritis: Analyses of Phase I and II Clinical Trials. Clin Pharmacokinet [Internet]. 2018 Aug 26;57(8):977–88. Available from: http://link.springer.com/10.1007/s40262-017-0605-6
37. Mohamed MF, Trueman S, Feng T, Anderson J, Marbury TC, Othman AA. Characterization of the Effect of Renal Impairment on Upadacitinib Pharmacokinetics. J Clin Pharmacol [Internet]. 2019 Jun 11;59(6):856–62. Available from: https://onlinelibrary.wiley.com/doi/10.1002/jcph.1375
38. Haubitz M, Bohnenstengel F, Brunkhorst R, Schwab M, Hofmann U, Busse D. Cyclophosphamide pharmacokinetics and dose requirements in patients with renal insufficiency. Kidney Int [Internet]. 2002 Apr;61(4):1495–501. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0085253815483723
39. Krens SD, Lassche G, Jansman FGA, Desar IME, Lankheet NAG, Burger DM, et al. Dose recommendations for anticancer drugs in patients with renal or hepatic impairment. Lancet Oncol [Internet]. 2019 Apr;20(4):e200–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30942181
40. Nadri QJ. Rituximab to treat active SLE in a hemodialysis patient. Saudi J Kidney Dis Transpl [Internet]. 2009 Nov;20(6):1085–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19861879
41. Iwamoto M, Honma S, Asano Y, Minota S. Effective and safe administration of tocilizumab to a patient with rheumatoid arthritis on haemodialysis. Rheumatol Int [Internet]. 2011 Apr 25;31(4):559–60. Available from: http://link.springer.com/10.1007/s00296-010-1430-5