



Rheumatologist's role regarding vaccination for COVID 19 in people with rheumatic diseases
https://doi.org/10.46856/grp.10.et096
Cite as:
Ferreyra Garrott LG, Pereira D, Lazaro MA, Graf C, Esposto A, Citera G. Rheumatologist's role regarding vaccination for COVID 19 in people with rheumatic diseases [Internet]. Global Rheumatology. Vol 2 / Jul - Dic [2021]. Available from: https://doi.org/10.46856/grp.10.et096
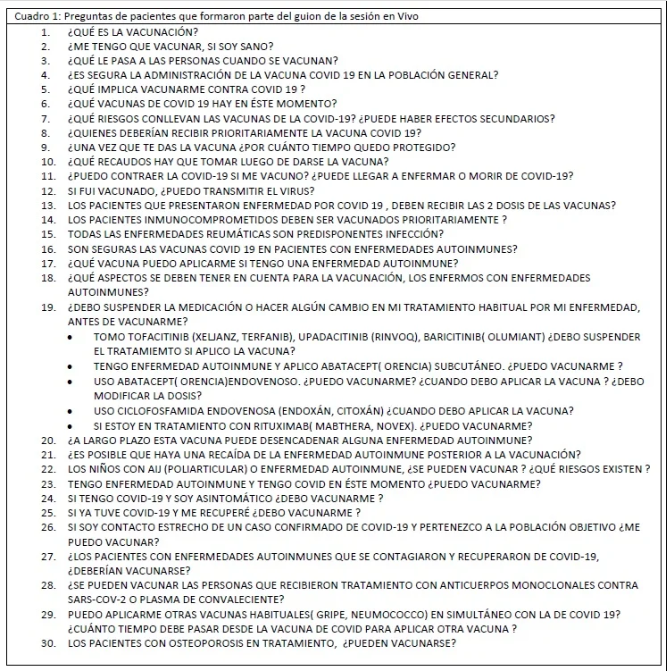
Table 1: Patient Questions Included in the Script for the Live Session
{kind=link}
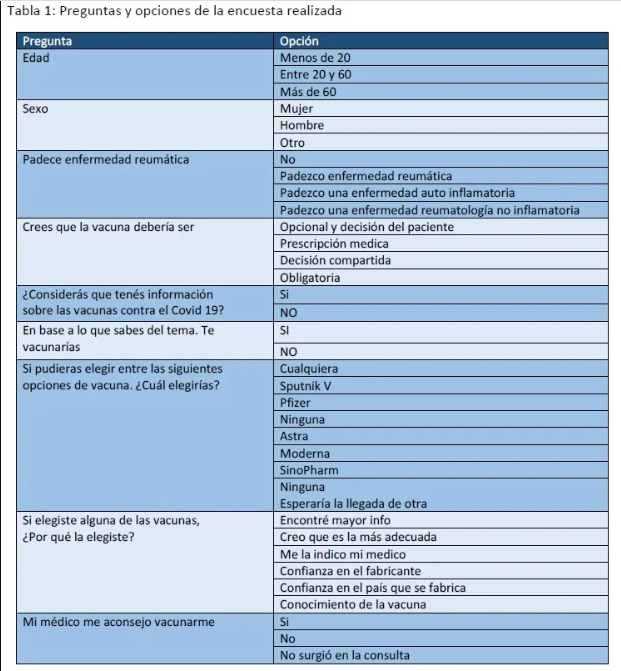
Table 1: Survey Questions and Answer Options
{kind=link}
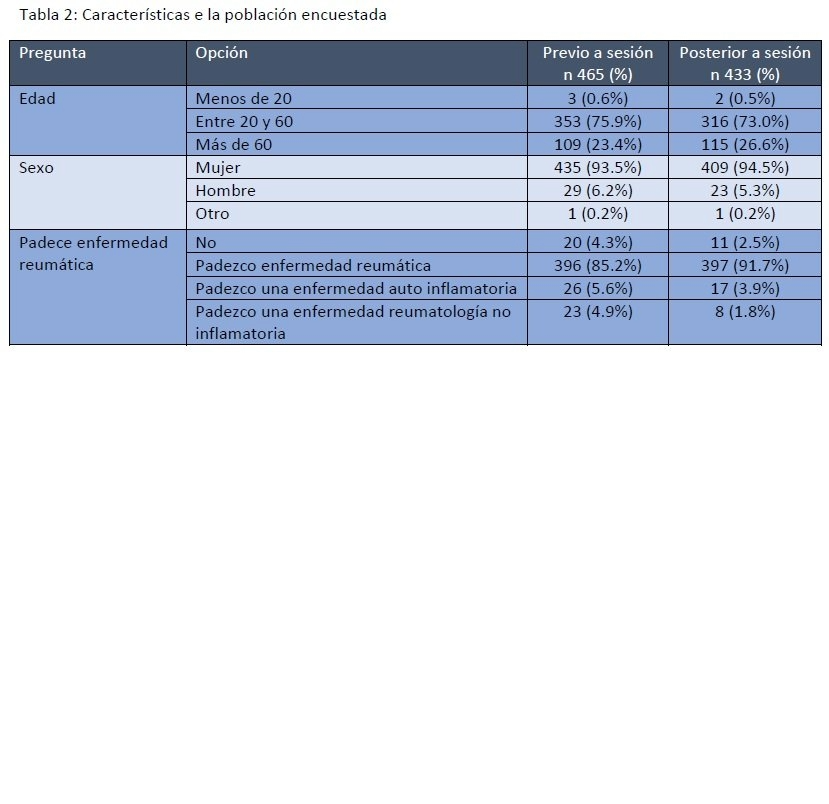
Table 2: Characteristics of the Surveyed Population
{kind=link}
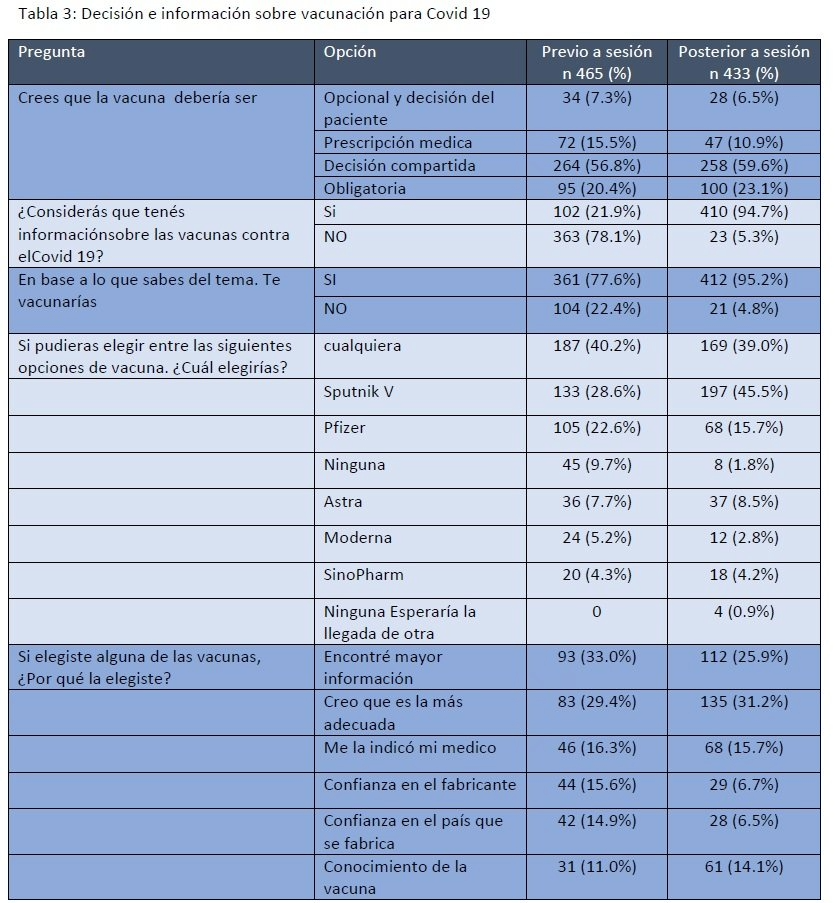
Table 3: Decision and Information Regarding COVID-19 Vaccination
{kind=link}
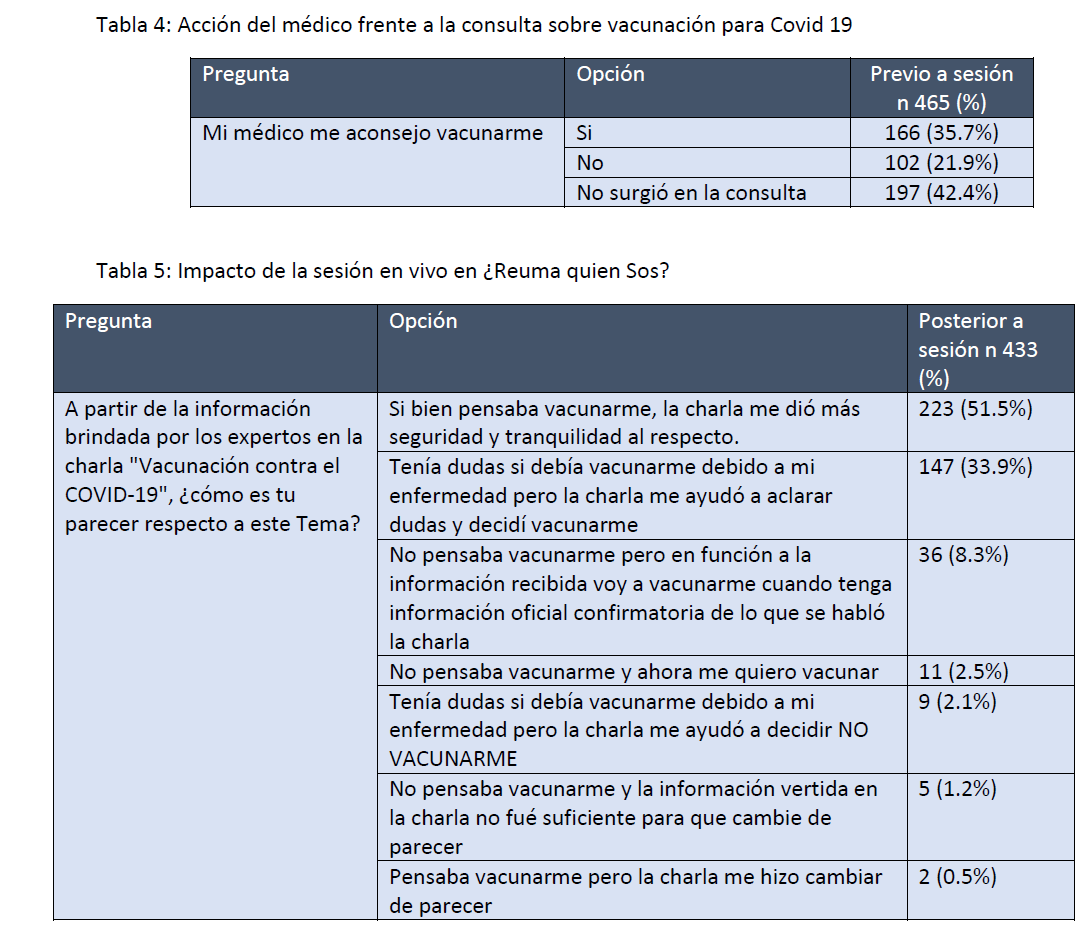
Table 4: Physician’s Response to Inquiries About COVID-19 VaccinationTable 5: Impact of the Live Session on “¿Reuma Quién Sos?”
{kind=link}
1301 Views
License
This is an open-access article distributed by the terms of the Creative Common Attribution License (CC-BY NC-4). The use, distribution or reproduction in other forms is permitted, provided the original author(a) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with this terms.
Rheumatologist's role regarding vaccination for COVID 19 in people with rheumatic diseases
Introduction: In the framework of vaccination against covid 19, patients with inflammatory, autoimmune or autoinflammatory rheumatic diseases and immunosuppressed had doubts about their situation. Experience with the different platforms is scarce.
Objective: Inform people with rheumatic diseases about vaccination for covid and measure the impact of the information.
Method: The Argentine Society of Rheumatology (SAR) organized a live information session on its portal for patients Reuma ¿Quién Sos?, to provide information on vaccination. Specialists in rheumatology and infectology participated, answered questions about vaccination for covid 19 in people with rheumatic diseases with information available so far, in addition, a brief survey was carried out before and after the session.
Results: 1900 people participated in the live session, there were 2400 comments, 997 reactions and it was shared 243 times. Within 7 days of the original post, the post reached 49,600 people. Before the session, 77% of those surveyed had considered getting vaccinated and at the end of the session this percentage increased to 95%, thus indicating an increase in acceptance of 22%. Prior to the session, only 35% received vaccination advice from their rheumatologist and 22% did not receive it at the time. When univariate analysis was performed for age, sex, and disease, no correlation was found with the survey questions.
Conclusion: The role of the scientific society and of the rheumatologist himself is fundamental in providing information on vaccination for Covid 19 in people with rheumatic diseases.
The COVID-19 pandemic caused by SARS-CoV-2 had a major impact on the lives of people, due to measures such as lockdowns, mobility restrictions, social distancing, the use of face masks, and sanitizing elements. The repercussions of these measures created the need to develop effective strategies to mitigate the impact on all aspects of people’s lives globally. With this objective in mind, researchers around the world worked to develop or optimize vaccines against COVID-19. Governments in each country adopted different strategic plans for both prevention and vaccination, acquiring vaccines from various producers, leading to unequal use and access to them in the region. In addition, the overwhelming flow of information on social media and the internet, often incorrect, caused confusion among the general population and especially among people with rheumatic diseases. For this reason, various scientific societies had to assume responsibility, take a stance, and generate recommendations for fellow physicians and their patients.
COVID-19 in Argentina
At the end of 2019, an outbreak of a new disease caused by coronavirus (COVID-19) occurred in Wuhan, China. There was rapid community, regional, and international spread, with an exponential increase in the number of cases and deaths. On January 30, 2020, the Director-General of the World Health Organization (WHO) declared the COVID-19 outbreak a public health emergency of international concern. The first case in the Americas Region was confirmed in the United States on January 20, 2020, and Brazil reported the first case in South America and the Caribbean on February 26, 2020; on March 3, the first case was detected in Argentina. Since then, COVID-19 has spread to all 54 countries and territories in the Region of the Americas (1).
Currently, as part of the national strategy to face this pandemic, Argentina is in the phase of “preventive and mandatory social distancing.” The goal is to recover the highest degree of normality possible in economic and social functioning, with all necessary precautions, and maintaining constant monitoring of the epidemiological situation (2). In Argentina, as of March 2021, a total of 2,905,172 confirmed cases and 62,599 deaths have been recorded (data from https://www.argentina.gob.ar/salud/coronavirus-COVID-19/sala-situacion). To mitigate the impact, the National Administration of Drugs, Foods, and Medical Devices (ANMAT) authorized different vaccines. Currently, the vaccination plan prioritizes essential personnel (health workers, teachers, security forces), older adults, and at-risk populations within these groups (3).
Patients with inflammatory, autoimmune, or autoinflammatory rheumatic diseases and immunosuppressed individuals expressed concerns about their eligibility for vaccination, as patients with these conditions were not included in most vaccine clinical trials and the overall experience with the different platforms is limited.
COVID-19 in People with Rheumatic Diseases
There are different types of rheumatic diseases. On one hand, a large group of them falls under degenerative diseases or those causing regional pain syndromes. These diseases do not pose a greater risk of COVID-19 infection compared to the general population. On the other end of the spectrum are autoimmune and autoinflammatory diseases with various organ involvements or those that require different levels of immunosuppressive treatment. Since the beginning of the pandemic, this latter group was considered at higher risk, although evidence from different studies remains ambiguous and not very robust (4). Moreover, various factors contribute to the prognosis of COVID-19 infection, including disease activity, treatment, organ involvement, and known risk factors for poor outcomes such as age, male sex, hypertension, cardiovascular disease, and chronic lung disease (5). In Italy, two studies showed ambiguous results depending on the diagnostic method. When swab tests were used, the prevalence of the disease was similar to the general population; however, when chemiluminescence testing was used, the risk of COVID-19 infection was higher in the rheumatic disease population (6,7). In this regard, the Global Rheumatology Alliance developed an international registry analyzing 3,729 people with rheumatic diseases worldwide, which showed that COVID-19 mortality was associated with higher disease activity and, as in the general population, with older age, male sex, and the presence of comorbidities (8).
Vaccination in People with Autoimmune and Autoinflammatory Rheumatic Diseases and Those on Immunomodulatory Treatment
There are four main platforms used by researchers to develop vaccines (9):
- Inactivated virus: CoronaVac (Sinovac Life Sciences, Beijing, China), New Crown COVID-19 (Wuhan Institute of Biological Products/Sinopharm), and BIBP-CorV (Beijing Institute of Biological Products/Sinopharm).
- Nucleic acid (RNA/DNA) vaccines: mRNA-1273 (Moderna/NIAID), BNT162b2 (BioNTech/Fosun Pharma/Pfizer), nCoVsaRNA (Imperial College London), INO-4800 (Inovio Pharmaceuticals/International Vaccine Institute). These have short development times and are low-cost.
- Viral vector vaccines: ChAdOx1 nCoV-19 (AstraZeneca/University of Oxford), Ad5-nCoV (CanSino Biological Inc./Beijing Institute of Biotechnology), Ad26.COV2-S (Janssen Pharmaceutical Companies), IIBR-100 (Israel Institute for Biological Research), Gam-COVID-Vac (Gamaleya Research Institute). These develop strong cellular and humoral immunity.
- Protein subunit vaccines: NVX-CoV2373 (Novavax), which require an adjuvant to generate a strong response.
Currently available in Argentina are: Gam-COVID-Vac (Sputnik V) (most available at the time of the live session), COVID-19 Vaccine ChAdOx1 nCoV-19 (Covishield), inactivated SARS-CoV-2 (vero cells) (Sinopharm), and ChAdOx1 nCoV-19 vaccine AZD1222 (AstraZeneca).
There is little evidence regarding the efficacy and safety of these vaccines in patients with rheumatic, autoinflammatory diseases, and those receiving immunomodulatory treatments. Based on experience with other vaccines, we know that the immune response may be somewhat lower compared to the general population (10,4). A recent German study compared antibody production after vaccination between people with immunosuppression due to chronic inflammatory diseases and the general population using mRNA vaccines. Despite the fact that only a small portion of the immunosuppressed group produced acceptable levels of antibodies, the adverse reactions were similar to those in the general population, and no disease flare-ups related to vaccination were observed (11).
Here is the English translation of your text, preserving the original meaning:
Given the limited experience regarding COVID-19 in rheumatic diseases—and even less so concerning vaccination—the Argentine Society of Rheumatology (SAR), through “¿Reuma Quién Sos?” (https://www.reumaquiensos.org.ar/), a website and social media initiative designed to provide information for patients with rheumatic diseases under the SAR, organized a live Facebook session with specialists in rheumatology and infectious diseases. The goal was to answer the most frequently asked questions from patients.
In the days leading up to the live session, promotional content was shared through social media, where patients were invited to submit their questions regarding “COVID-19 vaccination in patients with rheumatic diseases.” The data collected was used to create a script for the live session.
To assess the situation before and after the session, patients who participated were invited to complete a brief survey, designed to evaluate their views and knowledge about vaccination before and after the session.
A univariate analysis was performed using the survey questions as independent variables, and age, sex, and disease as dependent variables.
Aquí tienes la traducción al inglés del texto, manteniendo el contenido original sin cambios:
Three days before the live session, two posts were made on @ReumaQuienSos inviting patients to participate and submit questions for the specialists to answer. The members of the Patient Education Committee of the Argentine Society of Rheumatology (SAR) reviewed and grouped the patients' concerns into 30 questions to be addressed during the live session, generating a script of questions that were answered during the session by the invited specialists. (Table 1)
The live session took place on Tuesday, March 2, 2021, at 8:00 p.m. (Argentina time) via Facebook Live from the @ReumaQuienSos Facebook account. Moderators included CG, President of the Argentine Society of Rheumatology (SAR), MAL and LGFG, members of the SAR’s Patient Education Committee. The invited specialists were AE, an infectious disease specialist, and GC, a rheumatologist. The session lasted 1 hour and 40 minutes. A total of 1,900 people participated live, with 2,400 comments, 997 reactions, and 243 shares. The session followed the prepared question script, which was answered by the specialists.
465 people responded to the pre-session survey and 433 to the post-session survey. 75% of respondents were between 20 and 60 years old, and 94% were women. Around 58% stated that shared decision-making between doctor and patient was the best method for deciding on vaccination. (Tables 1 and 2)
Before the live session, 78% of respondents felt they did not have enough information about the vaccines and their illness in relation to vaccination. After the session, with the information provided, 94% felt they had enough information to make an informed decision about getting vaccinated. (Tables 3 and 5)
Prior to the session, 77% of those surveyed intended to get vaccinated, and after the session, this percentage rose to 95%, indicating a 22% increase in vaccine acceptance.
When considering vaccine preferences among patients, a significant increase was noted in favor of the Sputnik V vaccine, rising from 28.6% before the session to 45.5% after.
Before the session, only 35% had received advice from their rheumatologist about vaccination, and 22% had not received it due to not having had a consultation at the time of the survey. (Table 4)
A univariate analysis was conducted using the survey questions as independent variables and age, sex, and disease as dependent variables. No associations were found between the survey responses and these variables.
Aquí tienes la traducción completa al inglés, manteniendo fielmente el contenido original:
Educational activities for patients supported by a scientific society are a fundamental pillar in the treatment of chronic diseases.
In this unique pandemic situation, global uncertainty—driven by a high volume of information, the presence of fake news, and the variety of vaccines across different countries—led to growing misinformation among patients with rheumatic diseases, who were considered a high-risk group from the beginning of the pandemic.
In response to this, the Argentine Society of Rheumatology (SAR) decided to organize a live session with the aim of supporting and guiding patients regarding their situation in relation to COVID-19 vaccines.
Before the session, only 21.9% of respondents felt they had enough information to make a decision about getting vaccinated, although 77% were already willing to receive it. After participating in the session, the percentage of people who were satisfactorily informed and willing to be vaccinated increased to 94.7% and 95.2%, respectively.
To make decisions of this kind, the role of the rheumatologist is crucial. Before the session, 56.8% of patients, and after the session 59.6%, believed that the best way to make this decision was through shared decision-making with their rheumatologist. However, up to the time of the session, only 35.7% had received a recommendation to get vaccinated, and for 42.4%, the topic had not yet come up during consultations with their primary physician. It is worth noting that only two weeks before the session, the Argentine Ministry of Health had authorized the use of the vaccine for strategic personnel with these pathologies. Therefore, rheumatologists had very limited time to discuss this issue with their patients.
One important point to note is the increase in acceptance of the Sputnik V vaccine, which had previously raised uncertainty due to delays in data publication and skepticism rooted in political beliefs and media narratives, particularly among the general population and even more so among people with rheumatic diseases.
The data obtained from the session aligns with experiences in other countries. In a survey conducted in the Netherlands among 1,727 patients, of whom 1,361 had some type of rheumatic disease, 61% agreed with receiving the COVID-19 vaccine. Male gender (OR 1.7 [95% CI: 1.4 to 2.0]) and being over 60 years old (OR 2.0 [95% CI: 1.7 to 2.4]) were factors associated with willingness to be vaccinated. The main reasons for refusing vaccination were concerns about side effects and the limited time for vaccine development. The treating physician’s involvement in the vaccination decision proved important: among those with doubts, 69% of 515 patients, and among those initially opposed, 31% of 118, changed their minds based on their physician’s recommendation (12).
Another international study (Vaccinations Against COVID-19 – VAXICOV), which included Latin American participation, showed that more men than women were in favor of receiving the vaccine (71.2% vs. 52.3%, RR 0.93 [95% CI: 0.89–0.98]). Patients reported that the people they trusted the most to make vaccination decisions were specialist doctors (rheumatologists and general practitioners). When a doctor recommended vaccination, uncertainty decreased to 28.4% (360/1266) and unwillingness to be vaccinated dropped to 8.8% (111/1266) (13).
Here is the English translation, preserving the original meaning:
This experience highlights the importance of education and guidance for people with rheumatic diseases and the role that scientific societies play.
In recent years, patient-centered medicine has been considered a key approach, and educating patients is essential to provide them with tools that strengthen the doctor–patient relationship and allow them to make informed decisions about their health.
For these reasons, we believe that the role of the Scientific Society and the rheumatologist is fundamental in providing reliable information about COVID-19 vaccination for people with rheumatic diseases.
None of the authors has any conflict of interest related to this work.
No funding was received for this study.
1. PAHO. Respuesta de la OPS/OMS. 18 de enero del 2021. Informe n.o 41. 2021:1-11.
2. Presidencia de la Nación. Aislamiento social preventivo y obligatorio. Boletín Of la República Argentina. 2020:1-7. https://www.boletinoficial.gob.ar/detalleAviso/primera/227042/20200320….
3. Salud M De. Plan Estratégico Para La Vacunación Contra La Covid-19 En La. 2020.
4. Benucci M, Infantino M, Marotto D, Ardizzone S, Manfredi M, Sarzi-Puttini P. Vaccination against SARS-CoV-2 in patients with rheumatic diseases: doubts and perspectives. Clin Exp Rheumatol. 2021;39(1):196-202.
5. Ahmed S, Gasparyan AY, Zimba O. Comorbidities in rheumatic diseases need special consideration during the COVID‑19 pandemic. Rheumatol Int. 2021;41(2):243-256. doi:10.1007/s00296-020-04764-5
6. Emmi G, Bettiol A, Mattioli I, et al. Since January 2020 Elsevier has created a COVID-19 resource centre with free information in English and Mandarin on the novel coronavirus COVID- 19 . The COVID-19 resource centre is hosted on Elsevier Connect , the company ’ s public news and information . 2020;(January).
7. Benucci M, Damiani A, Giannasi G, et al. Serological tests confirm the low incidence of COVID-19 in chronic rheumatic inflammatory diseases treated with biological DMARD. Ann Rheum Dis. 2020;0(0):annrheumdis-2020-218214. doi:10.1136/annrheumdis-2020-218214
8. Strangfeld A, Schäfer M, Gianfrancesco MA, et al. Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann Rheum Dis. 2021:1-13. doi:10.1136/annrheumdis-2020-219498
9. Furer V, Rondaan C, Agmon- N, et al. Point of view on the vaccination against COVID-19 in patients with autoimmune inflammatory rheumatic diseases. 2021:1-10. doi:10.1136/rmdopen-2021-001594
10. Rondaan C, Furer V, Heijstek MW, et al. Efficacy, immunogenicity and safety of vaccination in adult patients with autoimmune inflammatory rheumatic diseases: A systematic literature review for the 2019 update of EULAR recommendations. RMD Open. 2019;5(2). doi:10.1136/rmdopen-2019-001035
11. Geisen UM, Berner DK, Tran F, et al. Immunogenicity and safety of anti-SARS-CoV-2 mRNA vaccines in patients with chronic inflammatory conditions and immunosuppressive therapy in a monocentric cohort. Ann Rheum Dis. 2021;(Cid):1-6. doi:10.1136/annrheumdis-2021-220272
12. Boekel L, Hooijberg F, van Kempen ZLE, et al. Perspective of patients with autoimmune diseases on COVID-19 vaccination. Lancet Rheumatol. 2021;9913(21):21-23. doi:10.1016/S2665-9913(21)00037-0
13. Felten R, Dubois M, Ugarte-Gil MF, et al. Vaccination against COVID-19: Expectations and concerns of patients with autoimmune and rheumatic diseases. Lancet Rheumatol. 2021;9913(21):21-23. doi:10.1016/S2665-9913(21)00039-4